SYSTEM: RESPIRATORY
FREQUENCY: ?
PATIENT HISTORY: This specimen comes from a 25 year old man who complained of numerous "attacks of bronchitis". On X-ray a cystic lesion was noted in the right lower lobe.
SPECIMEN R3-c26-0075
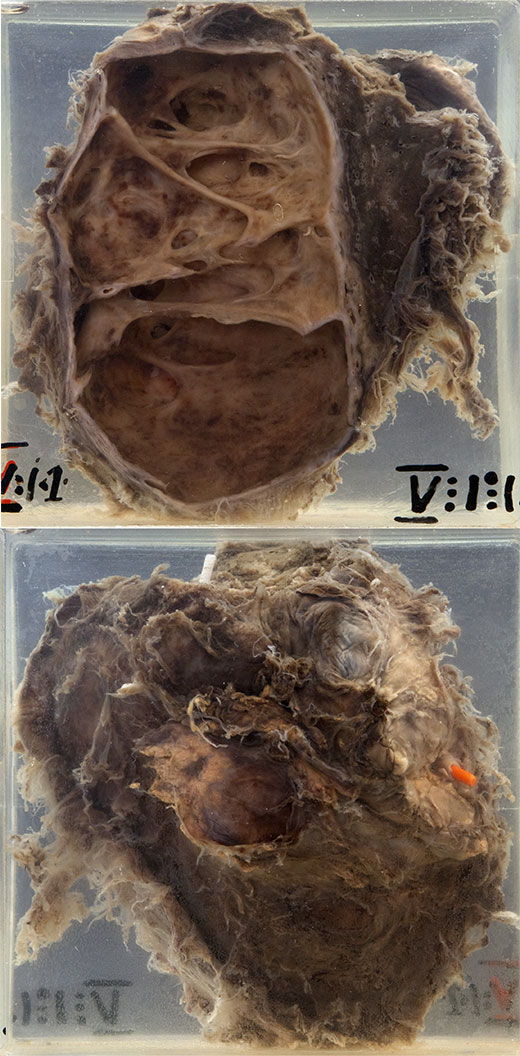
In the mounted specimen one sees a lobe of lung with dense pleural adhesions. At operation a large anomalous vessel was found passing to the medial aspect of the right lower lobe from the aorta. An abnormally situated vessel enters the medial surface of the lobe 8 cm from the hilum and is indicated by the orange probe. The greater part of the lobe is occupied by a large cystic cavity. This has thick fibrous walls and its internal surface is irregularly trabeculated. No communication could be demonstrated between the main bronchus to the lobe and the cavity. Histologically the cavity was lined, in the main, by bronchial epithelium but in places merely by granulation tissue or inflammatory exudate.
THE CONDITION:
A portion of lung is separated developmentally from the rest of the lung, does not communicate with the bronchial tree and has its own blood supply. The latter is usually in the form of a large artery arising from the aorta just above or just below the diaphragm. An intralobar sequestration is located within a normal lobe (almost always in the lower lobe) and lacks its own visceral pleura. An extralobar sequestration is located outside the normal lung and has its own visceral pleura. The intralobar type is more common. Extralobar sequestrations are more likely to be associated with other congenital anomalies.
Cases of intralobar pulmonary sequestration present at an older age than the extralobar sequestrations, and usually with recurrent localised infection. On X-ray a cystic area is seen within the lower lobe, often with fluid levels. Extralobar sequestrations are less likely to become infected and usually present as a subdiaphragmatic soft tissue mass. CT/MRI will often successfully delineate the lesion and in particular the aberrant blood supply, so avoiding more invasive techniques such as an arteriogram.
AETIOLOGY:
Extra and intra-lobar sequestrations probably arise by different maldevelopmental processes. Extralobar sequestrations are believed to evolve from an outpouching of the foregut which becomes separated from the rest of the developing lung (an "accessory lung"). Intralobar sequestrations probably arise secondary to anomalous vasculature.
PREVENTION & TREATMENT:
Sequestrations can be surgically removed, and this is generally recommended to avoid complications such as chronic infection or major haemorrhage.