
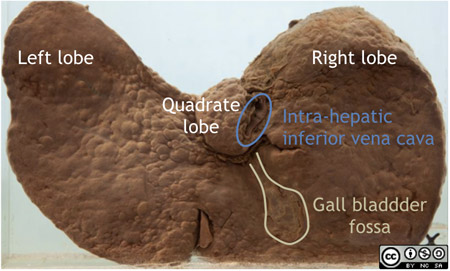
Inferior surface of the liver.

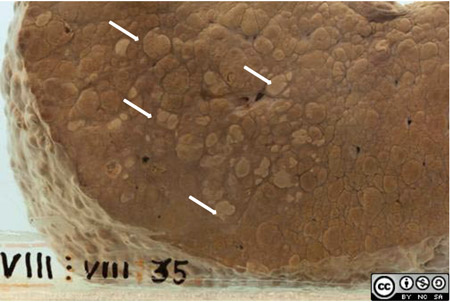
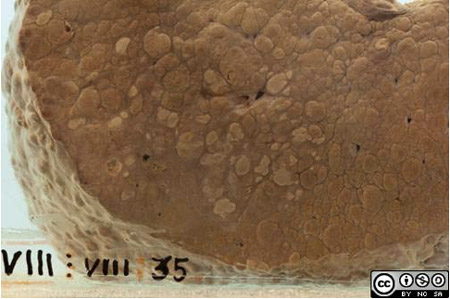
Cut surface of the liver.
Clinical data
- This patient was a 31 year old man with a 3 month history of abdominal swelling, epigastric pain, weight loss and jaundice.
- He drank 3 bottles of wine a day.
- On examination he had gross ascites and hepatomegaly.
- A week after admission he had an episode of haematemesis and gastroscopy showed that he was bleeding from oesophageal varices.
- Despite sclerotherapy he had repeated episodes of bleeding and developed signs of liver and respiratory failure.
Some laboratory investigations
- Chemistry
- albumin ↓
- AST and ALP ↑
- Total and conjugated bilirubin ↑
- Alpha-foeto protein ↑↑
- Virology
- Hepatitis B surface antigen positive
Pathology
- At autopsy the liver weighed 2530g (normal ± 1500g).
- It is diffusely riddled with nodules, compatible with cirrhosis.
- On the cut surface it can be seen that the nodules are mostly >3mm and up to 1cm in size, so this is predominantly a macronodular cirrhosis.
- A close up of an area in the right lobe shows that quite a few nodules have a suspicious fleshy appearance.
Histology
- Microscopy confirmed the macroscopic appearance of cirrhosis.
- In addition there was extensive replacement by poorly differentiated hepatocellular carcinoma.
A few notes on cirrhosis
- Cirrhosis is a response to diffuse injury of the liver parenchyma.
- It is characterised by two main processes
- constrictive fibrous scarring (fibrosis) and
- regenerative activity
which together result in the nodularity.
- The architecture of the entire liver and its vasculature is disrupted.
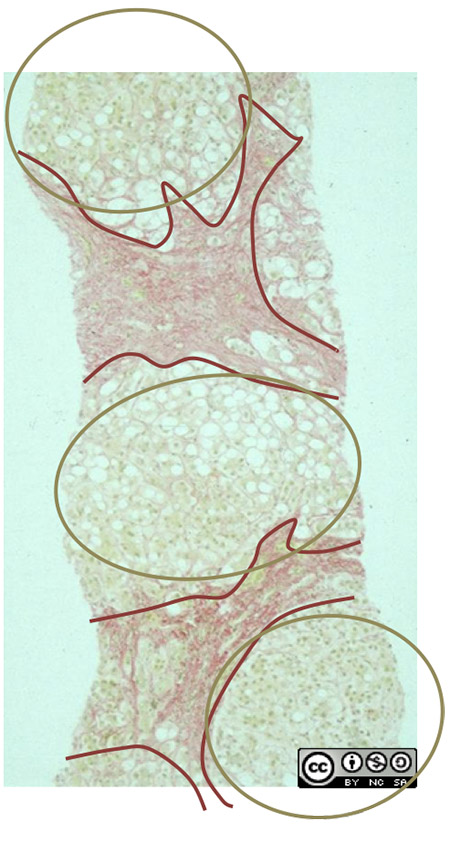
- This fragment of cirrhotic liver was sampled by liver biopsy.
- Fibrous septae (staining red) surround regenerative nodules of liver cells.
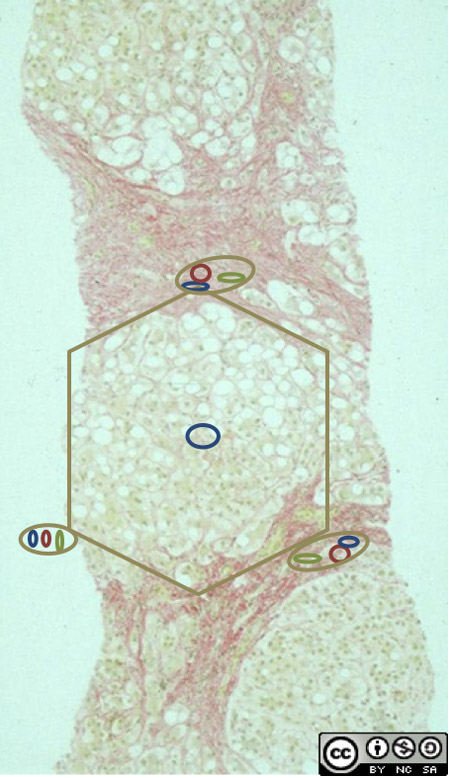
- The normal liver lobule structure is distorted.
- Portal tracts have largely been obliterated by the fibrosis.
- the obstructed portal circulation leads to portal hypertension.
- The central venule of each liver lobule has disappeared.
- the disrupted lobular circulation leads to hepatic dysfunction.
A few notes on hepatocellular carcinoma (HCC)

- HCC often presents as a single large liver mass
- or may have a multifocal origin, as in this case.
- It often but not always arises in a cirrhotic liver.
- Accumulation of DNA mutations during repeated cycles of regenerative cell division is an important factor in the pathogenesis of HCC.
Aetiology and local epidemiology
- The most important causes of both cirrhosis and HCC are alcohol and chronic viral hepatitis (B & C).
- Sub-Saharan Africa has historically had a high prevalence of hepatitis B (± 10%) and consequently a high incidence of HCC (29 per 100 000 in South Africa, 113 per 100 000 in Moçambique).
- In this context HCC presents in young adults (20 - 40 years, more often male) who have acquired hepatitis B in childhood or even in utero.
- The inclusion of the hepatitis B vaccine in the childhood immunisation programme in South Africa since 1995 will almost certainly reduce viral cirrhosis and HCC over time.
Related specimens in the collection
D9-g78-1712
A typical fatty liver from a patient with high alcohol intake. Early changes of cirrhosis were seen on microscopy.

D9-g78-1707
Predominantly micronodular cirrhosis typical of alcoholic liver disease.

D9-n83-1718
Hepatocellular carcinoma occurring as a single large nodule with a few daughter nodules.

References & links
- Kew, MC. Progress towards the comprehensive control of hepatitis B in Africa: a view from South Africa. Gut, 1996; 38 (Suppl 2):S31-S36
- To reinforce what you have learned here, look at the first 19 images of the section on Hepatic Pathology in WebPath http://library.med.utah.edu/WebPath/LIVEHTML/LIVERIDX.html#1