
Digital Pathology by University of Cape Town is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available at www.pathologylearningcentre.uct.ac.za.
Clinical data
-
The patient was a 27 year old man who died in 1948.
-
Three days before admission he had sudden onset of pleuritic pain on the right side of his chest.
-
He also had a cough with blood-stained sputum.
-
On examination he was flushed and pyrexial. His respiratory rate was increased and there were signs of marked consolidation of both the left and right lungs.
-
He died the day after admission despite large doses of penicillin.
Post mortem pathology
-
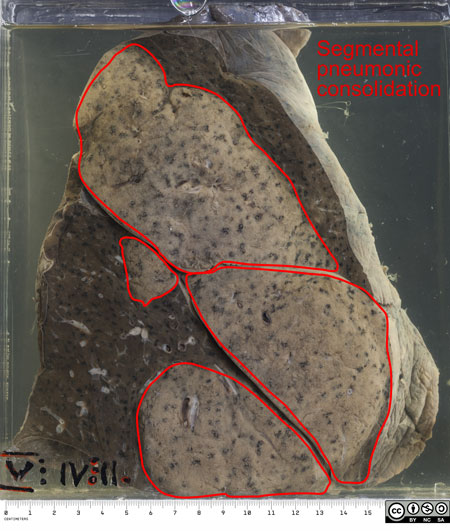
The specimen is his left lung which has been partially sectioned to show the grey-white areas of pneumonic consolidation.
-
These areas are not typically lobar (affecting the whole of a lobe) but rather lobular or segmental, that is affecting parts of the lobes.
-
This is said to be typical of Klebsiella pneumonia.
-
Another feature is that the affected areas appear to be swollen or bulging, which can give rise to the bulging fissure sign on x-ray. See https://radiopaedia.org/articles/bulging-fissure-sign
-
- There is a milky-looking fibrinous exudate on the pleural surface of the lung, seen here on the hilar aspect.

- No pneumonia can be accurately identified without microbiological investigation.
- A gram negative bacillus with culture characterisitics of Klebsiella pneumoniae was isolated from both lungs.

-
K. pneumoniae produces large, mucoid colonies after 24 hours of aerobic incubation. It is a lactose fermenter so on MacConkey agar the colonies are pink, as shown here.
-
The mucinous quality of Klebsiella would be noted by the pathologist at post mortem; the cut surface of the lungs appears mucinous and the knife used for sectioning would be sticky with mucous.
Some comments
-
Klebsiella pneumoniae and Klebsiella pneumonia are sometimes still called Friedländer’s bacillus and Friedländer’s pneumonia respectively, after the German physician Carl Friedländer, who described them in the 19th century.
-
Klebsiella pneumonia typically occurs in men over 50 years with an underlying chronic condition such as alcoholism or diabetes.
-
It is an aggressive pneumonia and has a tendency to progress to abscess formation.
-
When this patient fell ill in 1948 antibiotic options were limited. Today the first line antibiotic for community acquired Klebsiella pneumonia is coamoxiclav or a 3rd generation cephalosporin (cefotaxime or ceftriaxone).ââââââ