SYSTEM: GASTROINTESTINAL
FREQUENCY: 1 in 3000 live births
PATIENT HISTORY: No clinical or autopsy data are available for this case.
SPECIMEN D4-c21-0564
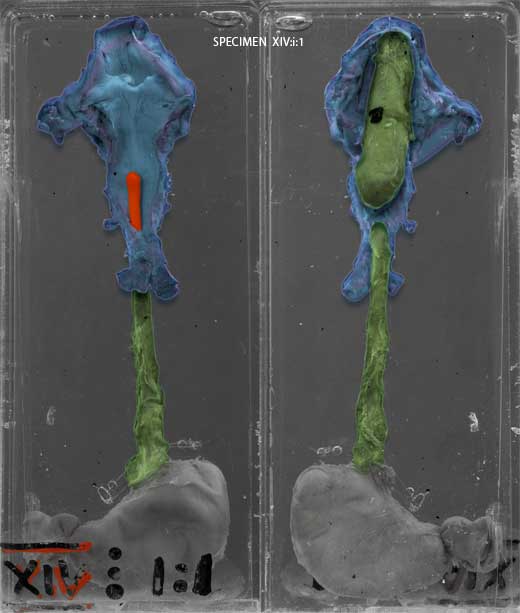
It can be seen that the upper part of the oesophagus ends blindly about 2cm below the epiglottis. The blind ending is dilated. The lower part of the oesophagus begins again just below, and it communicates with the trachea just above the bifurcation.

THE CONDITION
Oesophageal atresia is the absence of an oesophageal segment and is often associated with tracheo-oesophageal fistula . Tracheo-oesophageal fistula is an abnormal connection between the trachea and oesophagus. There are several variants of oesophageal atresia, with or without tracheo-oesophageal fistula. The specimen displayed here is by far the commonest type, that is where there is a fistula between the distal segment of oesophagus and the trachea.
Polyhydramnios is commonly seen in pregnancies where the foetus has oesophageal atresia, and about 1/3 of these babies are born prematurely. The earliest signs of oesophageal atresia / tracheo-oesophageal fistula in a newborn are excessive drooling of saliva, and attempts at feeding cause choking, regurgitation, coughing and cyanosis. Aspiration of saliva or gastric contents will cause pneumonitis if the condition is not recognised early enough. Inability to pass a gastric tube beyond 10 - 12cm is a strong clue, especially if the tube can be seen curled up in an oesophageal pouch on x-ray. If there is no tracheo-oesophageal fistula the abdomen will be scaphoid and there will be no stomach bubble on x-ray; conversely a distended abdomen and air in the stomach indicates a fistula.
Many children with oesophageal atresia / tracheo-oesophageal fistula have other congenital anomalies; in particular it may be part of the VACTERL (vertebral-anal-cardiac-tracheo-esophageal-renal-limb) association.
AETIOLOGY:
Embryologically the oesophagus and trachea both develop from the foregut. A tracheo-oesophageal septum is formed which separates the ventral trachea from the dorsal oesophagus. A disruption of this normal partitioning might explain oesophageal atresia and tracheo-oesophageal fistula, but other mechanisms have also been put forward. There is also abnormal development of the related neural plexuses and surrounding tissues, which contribute to the structural and functional defects of the trachea and oesopahagus in these patients even following repair.
PREVENTION & TREATMENT:
Healthy babies without other anomalies can have early surgery where the fistula is divided and the oesophagus anastamosed; survival is close to 100%. (The outcome in infants with multiple anomalies is much poorer.) In the longer term the child may have complications such as oesophageal dysmotility, dysphagia, reflux or stricture.
There is a low risk of recurrence of isolated oesophageal atresia / tracheo-oesophageal fistula within a family, 1% where a sibling is affected and about 4% if a parent is affected.