Research: Optimization and interpretation of serial QuantiFERON testing to measure acquisition of M. tuberculosis infection
SATVI researchers have co-authored “Optimization and interpretation of serial QuantiFERON testing to measure acquisition of M. tuberculosis infection” appearing in the American Journal of Respiratory and Critical Care Medicine.
Rational and study objectives: Conversion from a negative to positive QuantiFERON-TB test is indicative of Mycobacterium tuberculosis (Mtb) infection, which predisposes individuals to tuberculosis disease. Interpretation of serial tests is confounded by immunological and technical variability.To improve the consistency of serial QuantiFERON-TB testing algorithms and provide a data-driven definition of conversion.
Generally in practice, the interpretation of serial QuantiFERON-TB Gold in-tube tests, the gold standard for diagnosing latent M. tuberculosis infection, is complicated by immunological and technical variability.
In this study the analysis of large, independent cohorts provided immunological and epidemiological evidence that QuantiFERON-TB IFNy values between 0.2 and 0.7 IU/mL are confounded by immunological and technical variability.
Nemes et al.,2017.
In this study the analysis of large, independent cohorts provided immunological and epidemiological evidence that QuantiFERON-TB IFNy values between 0.2 and 0.7 IU/mL are confounded by immunological and technical variability. The study reports on optimized procedures to reduce variability, which are stricter than the manufacturer’s recommendations, as well as a more rigorous definition of QuantiFERON-TB conversion.
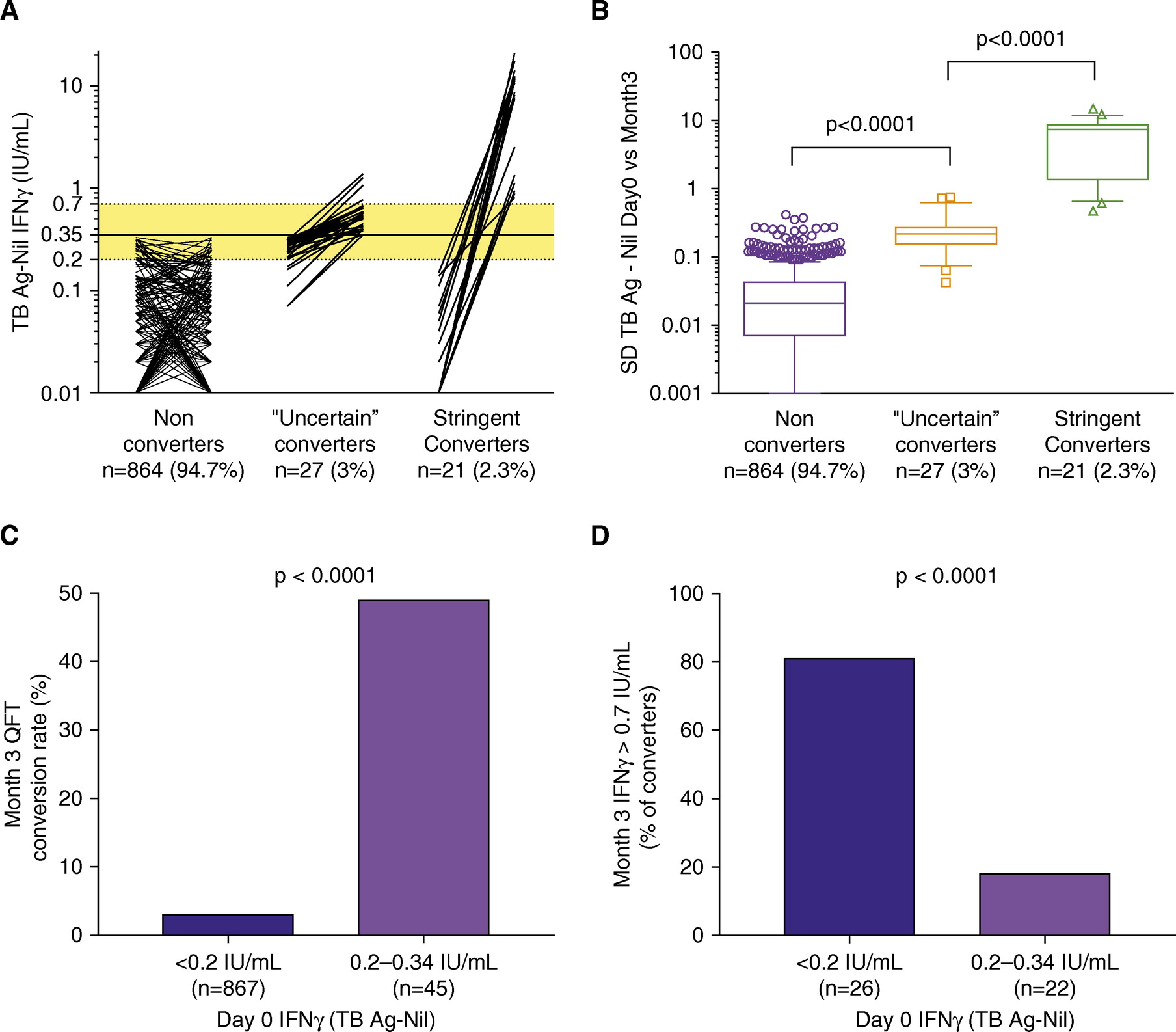
Figure Interpretation of serial QuantiFERON-TB Gold In-Tube (QFT) assays. IFN-γ values were measured in adolescents who were QFT negative at screening for the prevention of Mycobacterium tuberculosis infection trial (cohort 5) and retested 3 months thereafter (n = 912) to assess conversion rates in an endemic population. (A) Paired IFN-γ values, from left to right, for adolescents who did not convert (IFN-γ <0.35 IU/ml at both time points), those who converted with one of the two measurements falling in the uncertainty zone (“uncertain” converters), and those who converted from below to above the uncertainty zone (stringent converters). Dotted horizontal lines and yellow shading denote the uncertainty zone (0.2–0.7 IU/ml), and solid line denotes the assay cutoff (0.35 IU/ml). Zeros and negative values have been set to 0.01 to allow visualization on a logarithmic scale. (B) Variability across serial QFT assays, calculated as SD between IFN-γ values at Day 0 and Month 3 for each individual. Box-and-whisker plots denote median, interquartile range, and 10th–90th percentiles, respectively. P values were calculated by Mann-Whitney U test. (C) Month 3 conversion rates, stratified by IFN-γ values at Day 0. (D) Rates of converters with Month 3 IFN-γ values greater than 0.7 IU/ml, stratified by IFN-γ values at Day 0. In C and D, P values were calculated by Fisher’s exact test. Ag = antigen; TB = tuberculosis.
Implementation of optimized procedures and a more rigorous QuantiFERON-TB conversion definition (an increase from IFN-g ,0.2 to .0.7 IU/ml) would allow more definitive detection of recent Mtb infection and potentially improve identification of those more likely to develop disease.
These findings are important for the revision of guidelines for the interpretation of serial QuantiFERON-TB testing for clinical decision-making and for clinical trials in which acquisition of M. tuberculosis infection, defined by conversion of the QuantiFERON-TB assay, is a measure of vaccine efficacy.
Citation:Nemes E, Rozot V, Geldenhuys H, Bilek N, Mabwe S, Abrahams D, Makhethe L, Erasmus M, Keyser A, Toefy A, Cloete Y, Ratangee F, Blauenfeldt T, Ruhwald M, Walzl G, Smith B, Loxton AG, Hanekom WA, Andrews JR, Lempicki MD, Ellis R, Ginsberg AM, Hatherill M, Scriba TJ; C-040-404 Study Team and the Adolescent Cohort Study Team. Optimization and Interpretation of Serial QuantiFERON Testing to Measure Acquisition of Mycobacterium tuberculosis Infection. American Journal of Respiratory Critical Care Medicine, 196(5):638-648. Click here.