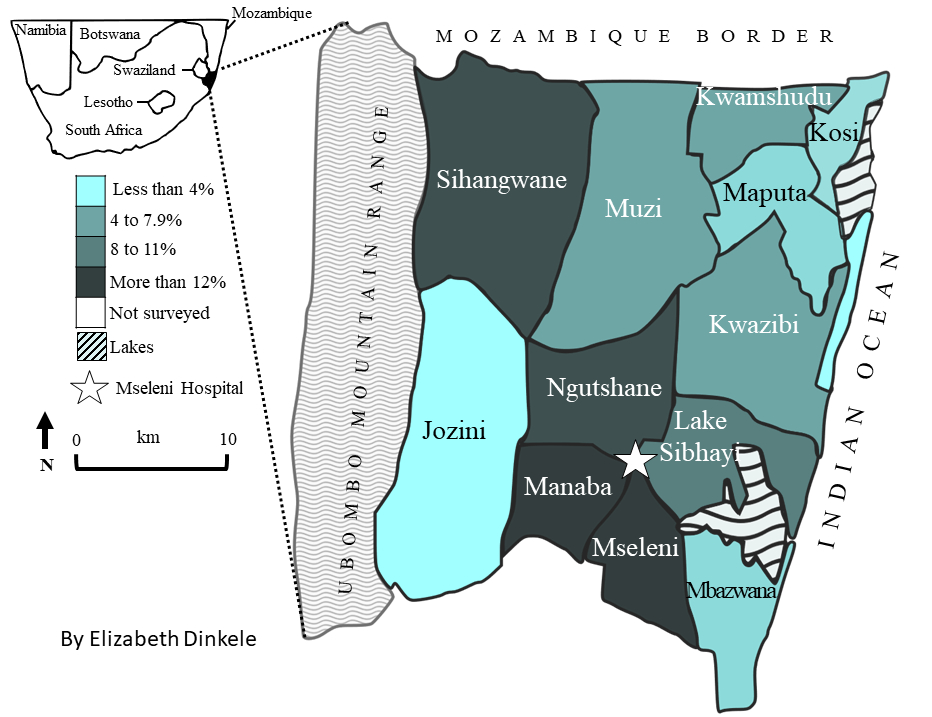
Mseleni joint disease (MJD) is a crippling osteoarthritis that is endemic to an area in the Maputaland region in KwaZulu Natal, South Africa. This rare disease is geographically confined to this isolated region and only affects people from a Bantu-speaking background and who are mainly of the Zulu culture. The geographic isolation of MJD is intriguing as the people of Mseleni are neither culturally nor genetically different from other people who live along the coastline in this region of South Africa (Nurse et al., 1974). MJD has been described as a bilateral, uniform arthropathy that is most severely localised to the hip. Diagnostic criteria remain vague due to variability in the severity and onset of joint pain. Consequently, the disease is usually identified at an advanced stage when patients are severely crippled, and treatment is limited to pain management and joint replacement.
MJD has been detected in children as young as six years old and is equally prevalent in both sexes until the age of 10. In adults this condition has been detected in 32-39% of the females and 10-11% of the males in the community (Fellingham et al., 1973; Yach and Botha, 1981). The higher prevalence in females may be attributable to migratory labour practices and cultural labour allocations that differ between the sexes.
Several potential cau

ses of MJD have been examined: environmental (soil, food, and water); geographic (climate and geology); diet (food, water, palm wine, preparation methods [fire wood and utensils], and nutritional deficiencies [vitamin and mineral]); autoimmunity; infectious agents; and genetics (genetic inheritance, collagen, serogenetics, and biochemical markers). Despite these avenues of ch, the cause for the condition remains unknown. The cause of MJD does not seem simple, but rather multi-factorial in character.
MJD is a chronic condition with a sweeping socio-economic impact on this community. It is a debilitating disease making daily chores difficult if not impossible depending on the severity of the condition. Many people in this region rely on their land for subsistence and inevitably depend on their families for survival. The impact is felt by y

oung people (especially young women) in the community who forgo school to help with familial care and subsistence. Research into the distribution and causes of MJD is needed to facilitate early interventions to reduce the burden of this disease on individuals and households to improve the quality of life and potentially contravene the cycle of disease, poverty and lack of education in this community.
Research Interest
As a post-doctoral student in South Africa at the University of the Witwatersrand, I worked on this disease, but my research was reinvigorated in 2012 by a collaboration with the late, Dr. Deepak Naryan (Yale University). Currently, an inter-disciplinary collaboration between Dr. Robea Ballo and I at the University of Cape Town (Cape Town, South Africa) with Dr. Victor Fredlund of the Mseleni Hospital (Mseleni, South Africa) is underway to provide a holistic understanding of MJD. Putative environmental and epigenetic risk factors are being explored using novel techniques from the fields of cell biology, genetics, epidemiology and biological anthropology.
Biological/Medical Anthropology
Expanding on my ear

lier research, Elizabeth Dinkele is a PhD candidate in my research group co-supervised by Dr. Ballo who is examining the distribution, and perceptions of MJD using epidemiological and anthropological techniques. She is investigating the link between MJD, socio-cultural/economic conditions in the region. In addition, she is providing an account of the beliefs, perceptions and experiences of MJD from patients and biomedical healthcare providers at the Mseleni Hospital. The overall aim of this research is to identify risk factors of MJD and make recommendations for enhancing treatment and health support. Our engagement with the Mseleni community transcends scientific research to address the disconnect between science and society through education and engagement of children and teenagers at the Christoff Meyer Maths and Science Institute in Mseleni.
Cellular Biology & Genetics
Dr. Robea Ballo from the Stem Cell Laboratory in the Department of Human Biology (UCT) leads the cell biology component of our investigation to better understand molecular pathogenesis of this disease. Her PhD was focused on MJD, returning to her roots, combined with her experience in generating patient-specific models of diseases from induced Pluripotent Stem Cells (iPSCs) is vital. Students in Dr Ballo’s team (Elizabeth Dinkele and Thulisa Mkatazo) have worked to reprogramme skin fibroblasts from MJD patients into iPSCs. Three-dimensional cartilage organoids differentiated from these iPSCs will be used to test the expression of genes suspected to be implicated in MJD. An MSc student, Thulisa Mkatazo, is testing the role of genes vital for cartilage development and maintenance. This work in generating cartilage organoids will be particularly useful to test cellular

responses of cartilage to various biological, molecular and physical stressors.
Publications
Dinkele ES, Ballo R, Fredlund V, Ramesar R, Gibbon V. 2020. Mseleni joint disease: an endemic arthritis of unknown cause. The Lancet Rheumatology 2(1): e8-e9. https://doi.org/10.1016/S2665-9913(19)30104-3
Gibbon VE, Harington JS, Penny CB. 2010. Mseleni Joint Disease: a potential model of epigenetic chondroplasia. Joint Bone Spine 77: 399-404 (rank 13/30; impact factor 3.218; citations: GS:6; WOS:3; S:4). https://doi.org/10.1016/j.jbspin.2010.01.013
Gibbon VE, Harington JS, Penny CB. 2010. La maladie de Mseleni: un modèle potentiel de chondrodysplasie épigénétique. Revue du rhumatisme 77: 430-435. (Translated from the English version in Joint Bone Spine). https://doi.org/10.1016/j.rhum.2010.05.006
Ballo R, Viljoen D, Machado M, et al. 1996. Mseleni joint disease- amolecular genetic approach to defining the aetiology. South African Medical Journal 86: 956–958.
